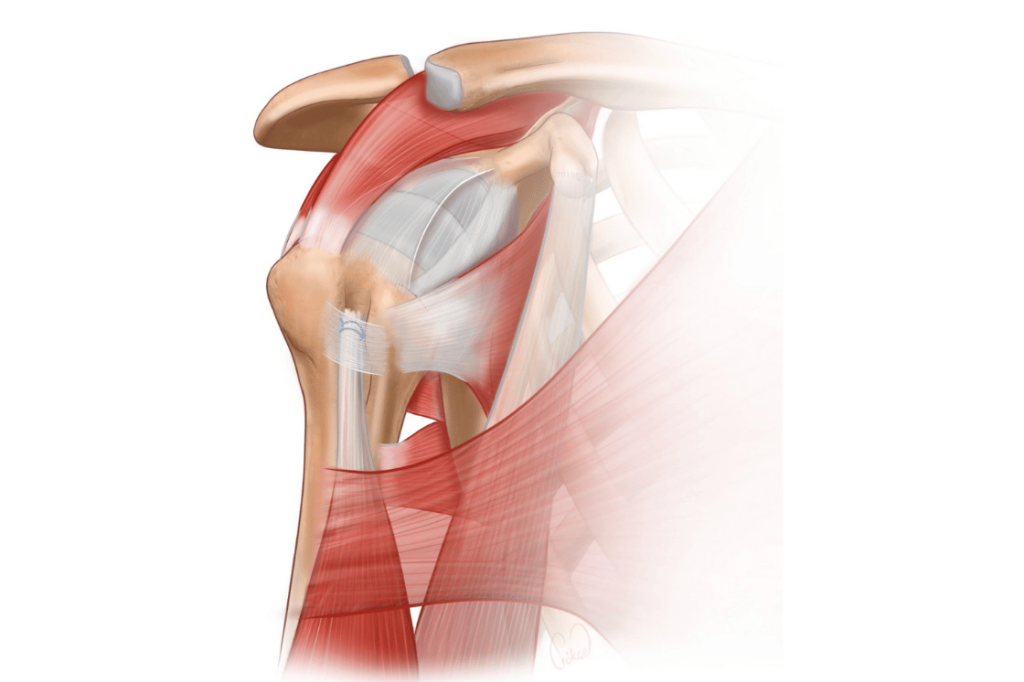
The biceps muscle is an important muscle group extending from the shoulder to the elbow, responsible for both bending the arm (flexion) and turning the palm upward (supination). This muscle is known to attach to the shoulder via two distinct tendons: the short head (attaching to the coracoid process) and the long head (extending into the glenoid, or shoulder joint). A proximal biceps tendon rupture typically occurs when this long head tendon tears.
These types of ruptures are most common in older individuals who have degenerative changes (age-related wear and tear) or chronic damage in their shoulder. At the time of the rupture, there may be a sudden “popping” sensation and pain in the shoulder. Subsequently, bruising may appear on the forearm, and the upward displacement of the muscle can create a characteristic “Popeye deformity” (a visible bulge in the upper arm). The loss of strength is generally mild; however, the aesthetic deformity and the potential for long-term pain can be bothersome to patients.
Some patients can maintain their quality of life with conservative treatment (non-surgical methods like rest and physical therapy). However, surgical treatment is often preferred for individuals with active lifestyles, patients concerned about the aesthetic deformity, and especially for younger or athletic patients.
Surgical treatment is performed by re-anchoring the ruptured long head of the biceps tendon to a new location on the upper arm bone (the humerus). This procedure is called a biceps tenodesis. It can be performed using an open or a mini-open technique. The tendon is securely fastened to the bone using special screws, suture buttons, or advanced suture systems.
Following surgery, short-term protection is provided with an arm sling, and physical therapy is then initiated without significant motion restriction. Most patients are highly satisfied with the outcome of the procedure, both functionally and cosmetically.