Shoulder fractures are common, especially in elderly individuals and patients with osteoporosis (a condition causing weak and brittle bones), often resulting from falls. These fractures occur in the head of the upper arm bone (humerus) and can sometimes be severely fragmented (broken into multiple pieces), seriously compromising the joint’s integrity. The treatment plan is determined based on the type of fracture, the degree of fragmentation, the patient’s age, and the condition of the shoulder’s soft tissues.
Traditionally, such fractures were treated with plate-and-screw fixation or a partial shoulder replacement (hemiarthroplasty). However, in recent years, reverse shoulder arthroplasty has become more prominent, especially for complex fractures and cases accompanied by problems with the rotator cuff muscles (the group of muscles and tendons stabilizing the shoulder).
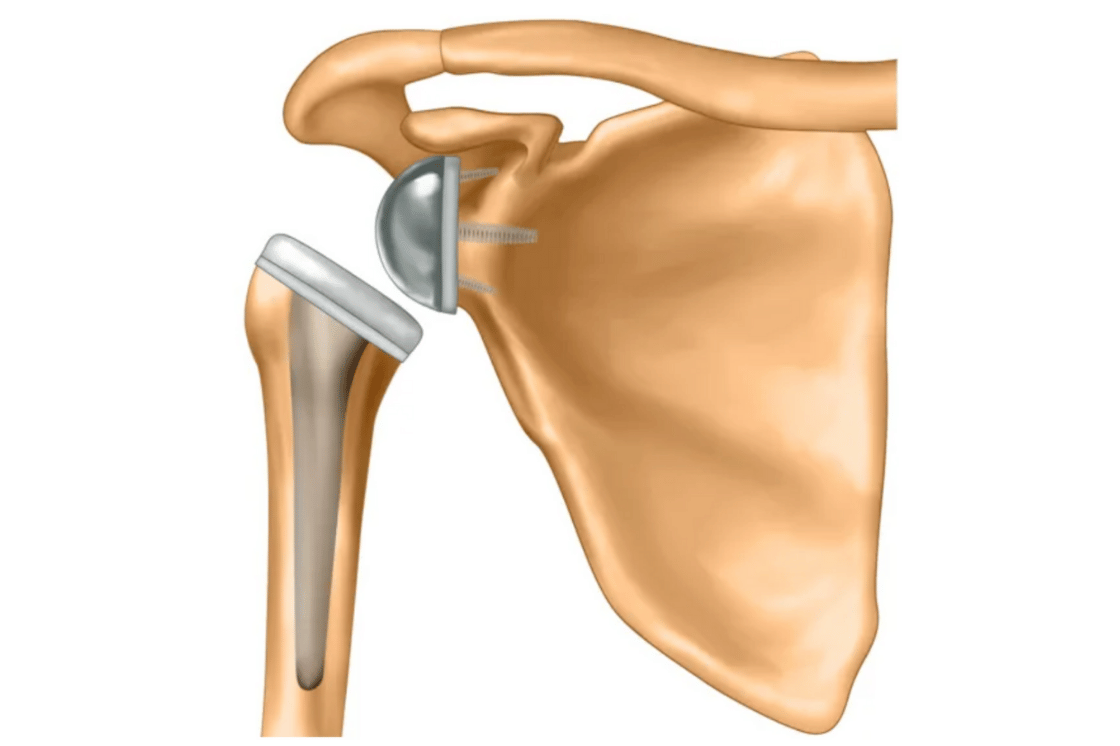
A reverse shoulder prosthesis is a special joint implant designed by reversing the shoulder’s natural anatomy. This design allows the deltoid muscle (the large muscle on the side of the shoulder) to power shoulder movements, even if the rotator cuff muscles are non-functional.
When Is Reverse Shoulder Arthroplasty Preferred?
Reverse shoulder arthroplasty is generally preferred in the following situations:
In these situations, a reverse prosthesis may be superior to hemiarthroplasty (partial replacement) in terms of both functional outcomes and pain reduction.