Supracondylar humerus fractures are among the most common elbow fractures seen in childhood. They typically occur in children aged 5–10 and are most often caused by falling onto an outstretched arm. These fractures happen in the part of the upper arm bone (humerus) closest to the elbow, near the growth plate. Because they are located around the joint, they must be managed carefully.
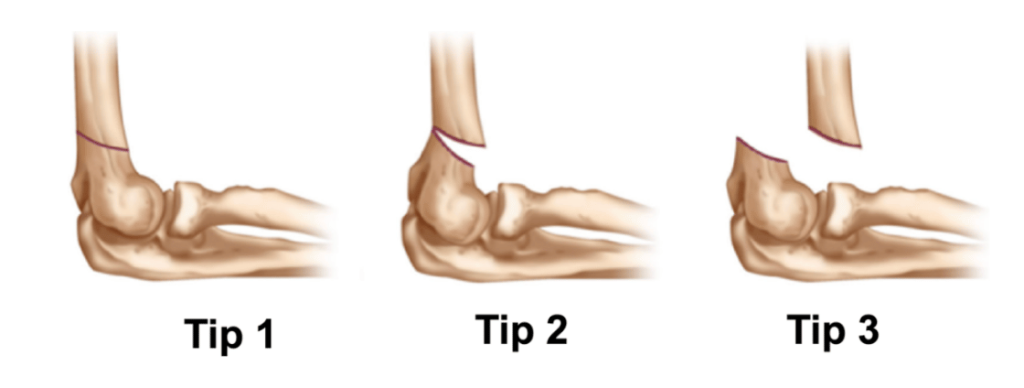
The treatment approach varies depending on the type of fracture and the amount of displacement (how far the bone pieces have moved). Fractures that are non-displaced or minimally displaced can be treated successfully with a cast, while displaced or angulated fractures may require surgical intervention. Surgery involves realigning the broken bone ends and securing them with small wire systems (K-wires).
If not treated correctly, these fractures can lead to deformity in the elbow’s angle, limited range of motion, or damage to nerves and blood vessels. Fortunately, with timely and appropriate intervention, children can overwhelmingly recover completely without any long-term complications (sequelae).