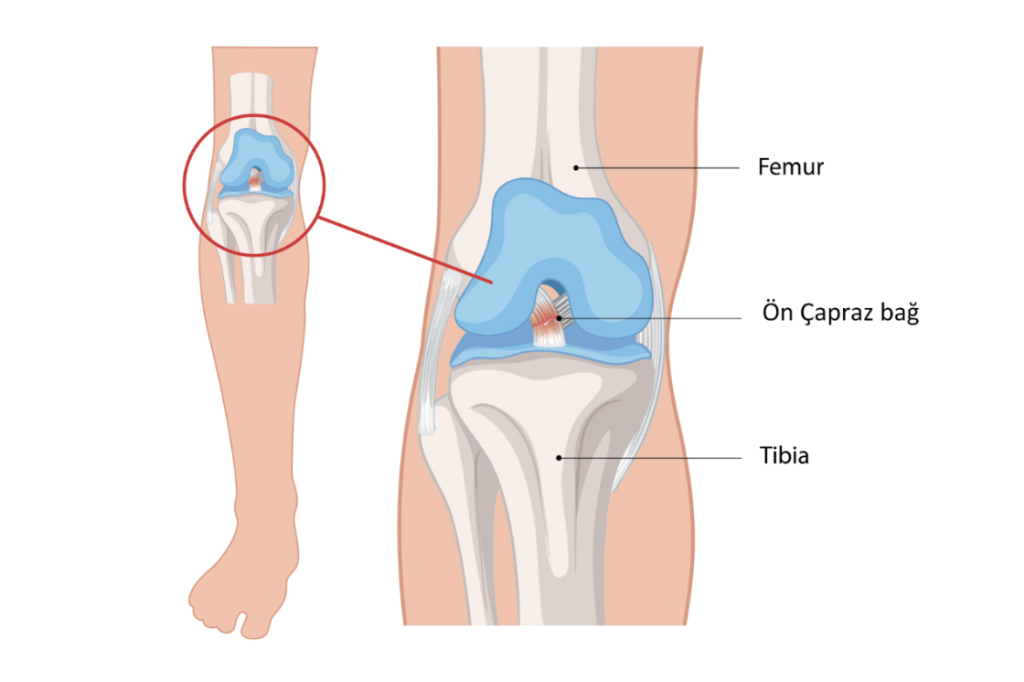
The anterior cruciate ligament (ACL) is a strong ligament located in the center of the knee joint, extending between the thigh bone (femur) and the shin bone (tibia). This ligament prevents the knee from sliding too far forward and controls unwanted movements during rotation (twisting). It can rupture, especially in athletes, during movements such as sudden changes of direction, stopping, jumping, or twisting the knee.
ACL tears are most common in sports that involve pivoting movements, such as football, basketball, and skiing. When the ligament ruptures, patients experience a “severe giving-way sensation” in the knee, along with sudden pain, swelling, and a loss of stability (the necessary tightness). Some patients report hearing a “popping or snapping” sound from their knee at the moment of the tear.
An ACL rupture seriously affects the mechanical stability of the knee. The treatment plan is determined based on the patient’s age, activity level, associated injuries (such as meniscus tears, cartilage damage, or other ligament injuries), and functional expectations. For patients who lead an active lifestyle or wish to return to sports, surgical reconstruction (rebuilding the ligament) is generally recommended.