The shoulder joint is one of the most mobile joints in the human body. This wide range of motion can, over time, cause the joint surfaces to wear down and the cartilage (the smooth tissue covering bone-ends) to deteriorate. This condition is called shoulder osteoarthritis, also known as “wear-and-tear” arthritis. As the osteoarthritis progresses, it results in shoulder pain, limited range of motion (stiffness), and difficulty performing daily activities.
Shoulder osteoarthritis is most commonly seen in individuals over the age of 50. The most frequent cause is age-related cartilage degeneration (the breakdown of joint-cushioning tissue). In addition, previous traumas (injuries), shoulder dislocations, rheumatic diseases (like rheumatoid arthritis), and rotator cuff tears can also lead to osteoarthritis in the shoulder joint. Over time, patients may find it difficult to perform simple actions such as putting on a shirt, combing their hair, or making overhead movements.
Conservative methods (non-surgical treatments) such as medication, physical therapy, and intra-articular injections (shots directly into the joint) may provide initial relief. However, in advanced-stage shoulder osteoarthritis, these methods become inadequate. When pain and limited motion become severe, total shoulder replacement surgery (also called total shoulder arthroplasty) is recommended.
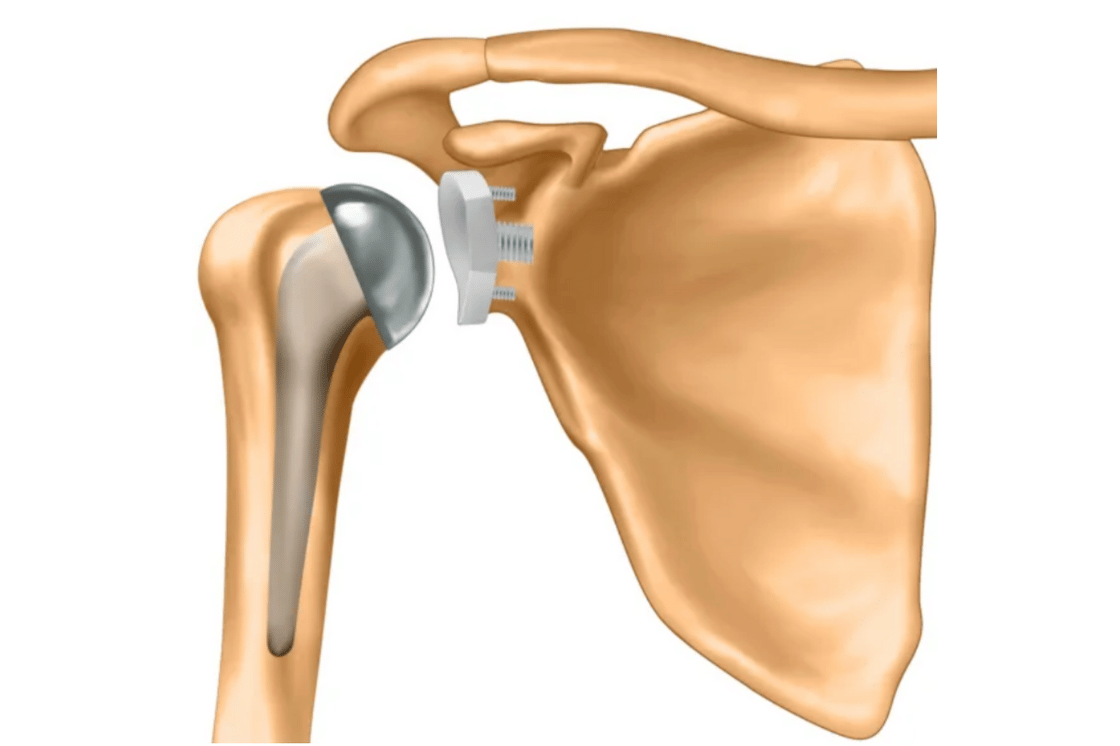
A total anatomical shoulder replacement involves replacing the damaged joint surfaces with an artificial joint (a prosthesis) made of metal and polyethylene (a medical-grade plastic) components. This prosthesis is designed to mimic the shoulder’s natural anatomy, which helps to reduce the patient’s pain and restore the shoulder’s range of motion. An anatomical prosthesis is the preferred option, especially for patients who have intact rotator cuff muscles.
Patients experience relief and a painless shoulder shortly after surgery. With a recovery process supported by physical therapy, the shoulder’s functions are largely restored. The success rate is significantly high with appropriate patient selection and the correct surgical technique.
