The olecranon is the prominent part of the ulna (forearm bone), located at the back of the elbow. The triceps muscle, which allows the arm to straighten, attaches to this bone. For this reason, olecranon fractures seriously affect elbow function. They usually occur as a result of a fall or direct trauma to the elbow.
Simple and non-displaced (where the bone pieces have not moved apart) fractures can often be treated with a splint or cast. However, in cases where the bone ends are separated (displaced), fragmented (comminuted), or disrupt the joint surface, surgical treatment becomes unavoidable. Surgical intervention is necessary both for the anatomical realignment of the bone and to restore the function of the triceps muscle.
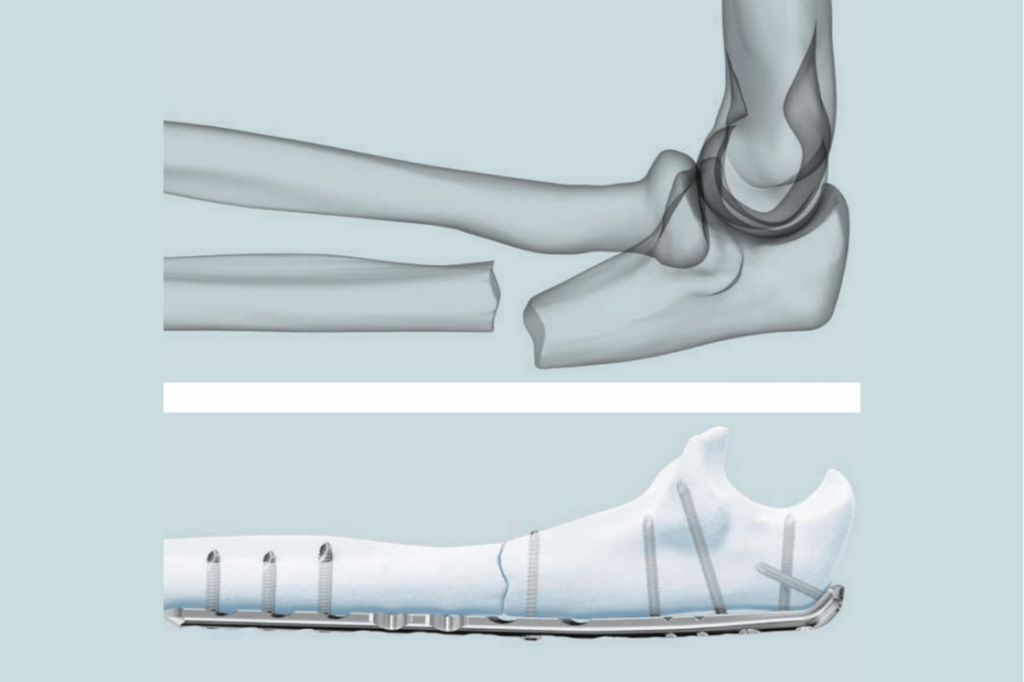
The most common methods used in the surgical treatment of olecranon fractures are:
The goal of these methods is to stabilize the fracture fragments, providing enough stability to allow for early motion. After successful surgery, most patients can regain their arm function in a short time.
